hEDS and MCAS Diet Tips: Navigating Elimination Diets When You Need More Than One
hEDS doesn't just affect joints. The same connective tissue differences that cause hypermobility also impact the gut. The entire digestive tract is made of connective tissue, so when that tissue is too stretchy, peristalsis weakens — causing slow digestion, discomfort, nausea, vomiting and constipation. Up to 75% of people with hEDS have functional gastrointestinal disorders, including gastroparesis and chronic constipation. The stomach empties slowly. The colon moves at a fraction of the normal pace.
Many hEDS patients also have mast cell issues — some have mast cell activation syndrome (MCAS), others have histamine intolerance or mast cell-related symptoms that don't meet the full diagnostic criteria. So on top of the usual fatigue, brain fog and pain, histamine in foods can trigger flushing, joint pain, and a cascade of inflammatory responses that make everything worse.
Bodies in pain need energy to recover. Hypermobile bodies are estimated to use significantly more energy just to maintain posture and stability — the muscles have to compensate constantly for ligaments that don't do their job. Research shows adults with hEDS have 30–49% lower muscle strength despite normal muscle mass, because those muscles are working overtime. But the nourishing food these bodies need can often become a source of pain and anxiety rather than nutrition and pleasure.
Autonomic Dysfunction and the Gut
Autonomic issues further compound hEDS gut problems. The same dysautonomia that gives many of us POTS also worsens digestion. An overactive sympathetic nervous system — stuck in fight or flight — deprioritises digestion. The gut slows down, nausea increases, gastric emptying delays. POTS has been identified as an independent predictor of GI dysmotility in hEDS patients, and in studies, over 76% of hEDS patients tested for dysmotility had some form of it.
When your nervous system is telling your body there's a threat, digesting food is the last thing it wants to do.
Slow Transit, SIBO and Fermentation
Because of weak peristalsis and gastroparesis, food sits in the digestive system for longer than it should. That prolonged transit causes discomfort, bloating, and fermentation — and it creates the ideal conditions for small intestinal bacterial overgrowth (SIBO). SIBO is significantly associated with IBS and functional constipation, and treating it in the context of hEDS is particularly challenging because the underlying motility issues don't resolve. Low FODMAP and SCD diets are often introduced to help reduce symptoms, clear SIBO, and manage the bloating, gas and pain that come with it.
Inflammation and the First Things to Go
Gluten and lactose are usually the first things patients are told to eliminate because of their inflammatory effects. Gluten triggers an immune response in many people with compromised guts, and lactose becomes harder to digest as chronic inflammation disrupts the gut flora needed to break it down. Both are also fermentable — high FODMAP, problematic on SCD — so they compound the bacterial overgrowth and motility issues already in play.
The hEDS-MCAS-Diet Connection
This is something that doesn't always get explained well in clinical settings: hEDS and MCAS frequently co-occur. Some estimates suggest up to 25% of hEDS patients have MCAS, and a much higher proportion have some level of mast cell involvement. The leading theory is that the disrupted collagen in hEDS physically irritates the mast cells that reside in connective tissue, causing them to degranulate — releasing histamine and other substances that trigger symptoms throughout the body.
Combine that with the slower gut transit that comes with hEDS, and histamine-rich foods sit in the system for longer, amplifying the reaction. Foods that most people consider healthy — aged cheeses, fermented vegetables, avocados, tomatoes — can become genuinely problematic. You can compare overlapping elimination diets to see where these conflicts sit across different protocols.
Restricted Intake
It's easy to see how hEDS patients end up on a very restricted diet. And many of us, seriously underweight.
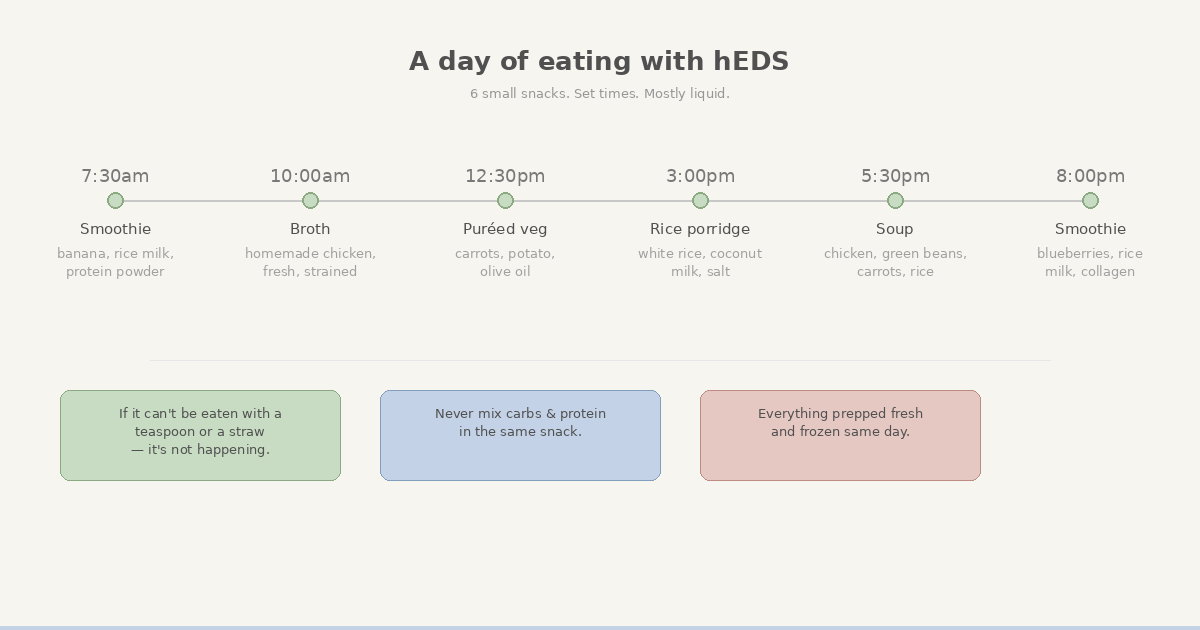
I've lived off the same, very limited range of foods for years now. I also find solids problematic no matter how much I chew, so about 90% of my diet is liquid or mush. My basic rule — if it can't be eaten with a teaspoon or a straw, it's not happening.
The concept of meals is also foreign to me and many other hEDS sufferers. Small snacks cause less discomfort and digest more quickly than larger, more substantive meals. I eat six times a day, at set times. Eating food groups separately — never mixing carbs and protein — has also helped.
I can't easily socialise around meals, coffees, or anything that involves sitting in a restaurant. I can't travel much. There's nothing I can buy out or get in a restaurant, so I meal-prep the same foods every single day. I miss out on the social occasions that inevitably centre around food — casual dinners out to Christmas lunches with family.
It's a way of living that only people going through it can fully appreciate.
It helps physically, even if it's hard emotionally. I still don't look forward to food, but the pain associated with it has reduced. It's a trade-off — restriction for function — or sociability and pain.
The Hardest Part: Finding Reliable Information
Managing multiple elimination diets takes serious motivation and willpower. The food decision fatigue alone is a fight we don't need on top of everything else.
Histamine levels vary depending on how food is stored and for how long. Cooking methods change FODMAP content. Ripeness affects histamine in fruit and vegetables. Different countries' low-FODMAP guidelines don't always align. Brands vary too. When multiple restrictions are layered together, you just need to know which foods are good to go and which are not.
I spent months cross-referencing apps, spreadsheets, and blog posts. I'd think something was safe, eat it, and spend the next day dealing with the consequences. I knew about food to start with, but the learning curve was still steep — and navigating it while already managing the rest of my symptoms was not fun.
I couldn't find a single tool that understood overlapping elimination diets. So I built one — how ClearToEat cross-references elimination diets.
What Actually Helps
Consolidate your information. Having one source that covers all your diets and how they intersect saves time and cognitive load. Jumping between five separate apps is exhausting and error-prone.
Track what works for your body. General food lists are only ever a starting point. Individual tolerance varies a lot — especially with hEDS and MCAS. The only way to know what works is systematic elimination and careful reintroduction.
Build a sustainable rotation. Within my restrictions, I've found about twenty foods I can eat routinely, plus a few I can manage small amounts of on occasion. Having a concrete list of what I can eat — rather than just what I can't — makes a real difference.
Stay connected and stand your ground. This is genuinely the hardest part. When food is central to socialising and you can't participate in the same way, it's easy to withdraw. Or ignore your needs and suffer the consequences. It really sucks watching everyone else enjoy nice meals and having to explain why you can't participate — but it's better than isolating yourself. Or dealing with the fallout of ignoring your needs.
---
FAQ
Why do people with hEDS have so many food issues?
The same connective tissue differences that cause hypermobility affect the gut wall, leading to slow transit, dysmotility, and functional GI disorders in up to 75% of hEDS patients.
What is the connection between hEDS and MCAS?
Irregular collagen in hEDS can irritate mast cells, triggering histamine release. Around 25% of hEDS patients have co-occurring MCAS, which adds histamine dietary restrictions on top of existing GI issues.
What diets help with hEDS GI symptoms?
Low FODMAP is commonly recommended for IBS-type symptoms. If MCAS is present, low histamine is added. Many patients end up on 3-5 overlapping diets.
Is there an app for managing hEDS and MCAS dietary restrictions?
ClearToEat was built by someone with hEDS and severe GI issues, specifically to cross-reference multiple elimination diets in one search.
This is a personal account of living with hEDS and managing multiple elimination diets. It's not medical advice — dietary needs vary significantly between individuals. Work with a registered dietitian familiar with hEDS and MCAS to develop a plan that's right for you.